Babesiosis is commonly labeled as a tick-borne disease, but in clinical practice it behaves more like a chronic blood-borne infection with multiple transmission routes, including vertical transmission. Successful management depends on recognizing these realities and applying a practical treatment protocol using locally available drugs.
⚠️ Atovaquone is NOT readily available in the Philippines, so treatment protocols must rely on Imizol (imidocarb dipropionate) and combination antibiotic therapy.
CLINICAL PEARL #1: Babesia Is Not Always Tick-Borne
Aside from ticks, Babesia can be transmitted via:
- Vertical (transplacental) transmission
- Blood transfusion
- Shared needles or contaminated instruments
- Dog bites with blood exposure
➡️ Puppies may be infected in utero, even with zero tick exposure.
CLINICAL PEARL #2: Vertical Transmission Can Cause Fading Puppy Syndrome
Babesia can cross the placenta from dam to puppies.
Common presentations in puppies:
- Pallor
- Weakness, poor suckling
- Failure to thrive
- Unexplained anemia or thrombocytopenia
- Sudden death
The dam may appear clinically normal or only mildly affected.
➡️ Always consider Babesia in anemic or failing puppies, especially when multiple littermates are affected.
CLINICAL PEARL #3: Babesiosis May Be Acute, Chronic, or Subclinical
- Acute: fever, hemolytic anemia, hemoglobinuria
- Chronic: intermittent lethargy, weight loss, mild anemia
- Subclinical carriers: normal exam, PCR positive (if available)
Stressors such as surgery, pregnancy, illness, or immunosuppression can reactivate latent infection.
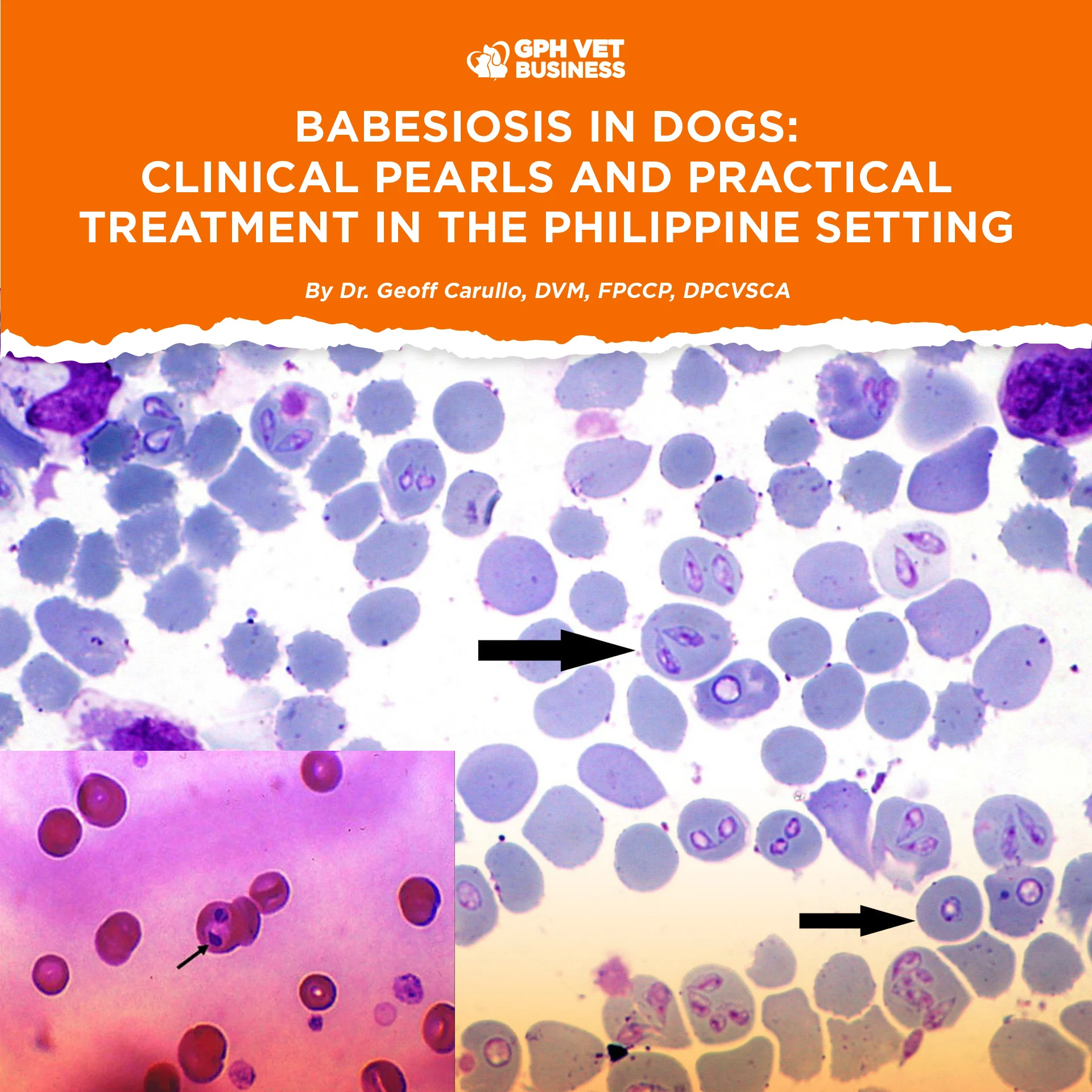
CLINICAL PEARL #4: Blood Smear Negativity Does NOT Rule Out Babesia
- Parasitemia may be extremely low
- Chronic cases are often smear-negative
- PCR is more sensitive but not always accessible
Clinical judgment is essential.
FIRST RULE OF TREATMENT: STABILIZE THE PATIENT
Do not rush antiparasitic therapy in unstable patients.
Stabilize first if:
- PCV < 20%
- Severe thrombocytopenia
- Hypoglycemia, dehydration, or shock
Supportive care:
- IV fluids
- Blood transfusion if PCV < 15–18% or clinically indicated
- Oxygen therapy when needed
MAIN ANTIPARASITIC THERAPY: IMIZOL (Imidocarb Dipropionate)
Dosage:
- 6.6 mg/kg IM, deep intramuscular
- Single dose
- May repeat once after 14 days if response is incomplete
Premedication (IMPORTANT):
Atropine sulfate 0.02–0.04 mg/kg IM or SQ
Give 15–30 minutes before Imizol to reduce cholinergic side effects.
⚠️ Imizol improves clinical disease but does not guarantee complete parasite clearance, especially in Babesia gibsoni infections.
WHEN IMIZOL ALONE IS NOT ENOUGH
(Chronic, Relapsing, or Partial Responders)
OPTION 2: COMBINATION THERAPY
(No atovaquone – Philippine-appropriate protocol)
This protocol is recommended for:
- Chronic or relapsing babesiosis
- Suspected carrier state
- Vertical transmission cases
- Incomplete response to Imizol alone
🔹 Clindamycin
Dose:
25 mg/kg PO q12h
Duration:
✅ 28 days
Role:
- Backbone of combination therapy
- Reduces parasitemia
- Helps control chronic infection
⚠️ Do NOT shorten duration. Underdosing increases relapse risk.
🔹 Doxycycline
Dose (choose one):
- 5 mg/kg PO q12h
- OR
- 10 mg/kg PO q24h
Duration:
✅ 21–42 days (case-dependent)
Role:
- Addresses concurrent tick-borne infections
- Reduces inflammatory burden
- Supports recovery but is not curative alone
Give with food or water to reduce esophagitis risk.
🔹 Metronidazole
Dose:
10–15 mg/kg PO q12h
Duration:
✅ 10–14 days ONLY
Role:
- Immunomodulatory support
- Useful in chronic or relapsing cases
⚠️ Avoid prolonged use due to neurotoxicity risk.
PRACTICAL TREATMENT TIMELINE
- Day 0: Stabilize → Atropine → Imizol 6.6 mg/kg IM
- Day 1–28: Clindamycin
- Day 1–21 to 42: Doxycycline
- Day 1–10/14: Metronidazole, then discontinue
CLINICAL PEARL #5: Avoid Steroids Unless Absolutely Necessary
Babesiosis can mimic IMHA.
- Steroids may worsen parasitemia
- Rule out Babesia before labeling anemia as immune-mediated
- If unavoidable, use lowest effective dose and combine with antiparasitic therapy
MONITORING PLAN
- PCV/HCT every 24–48 hours initially
- Platelet count when available
- Monitor appetite, activity, and relapse
Recovered dogs should not be used as blood donors.
FINAL CLINICAL TAKEAWAY
In the Philippine setting:
- Atovaquone is not an option
- Imizol remains the cornerstone
- Combination therapy reduces relapse
- Doxycycline often requires 21–42 days
- Vertical transmission is real and clinically significant
- Babesiosis is managed, not always eradicated.
Sharing this helps others understand what it really means to be a vet. Like and follow if you’re with us.