Blood parasitism remains one of the most common yet diagnostically challenging conditions in small animal practice, particularly in endemic regions.
Clinicians frequently encounter:
- Discordant test results
- Subclinical infections
- Chronic hematologic abnormalities without definitive confirmation
The increasing availability of PCR has led to the perception that it is the “gold standard.” However, this assumption must be interpreted in the context of parasite biology, host response, and real-world clinical limitations.
COMMON CANINE BLOOD PARASITES
In practice, the most relevant pathogens include:
- Ehrlichiosis (Ehrlichia canis)
- Anaplasmosis (Anaplasma spp.)
- Babesiosis (Babesia spp.)
- Hepatozoonosis (Hepatozoon spp.)
Each organism exhibits different:
- Tissue tropism
- Circulation patterns
- Immune dynamics
These differences directly influence diagnostic outcomes.
WHAT ARE WE REALLY DETECTING?
A critical but often overlooked point:
– Most blood parasite lateral flow kits used in practice are antibody-based tests.
This is especially true for:
- Ehrlichia
- Anaplasma
- Babesia
But not true for Dirofilaria immitis.
Meaning:
– A positive rapid test = evidence of exposure and immune response
– Not necessarily active infection
In contrast:
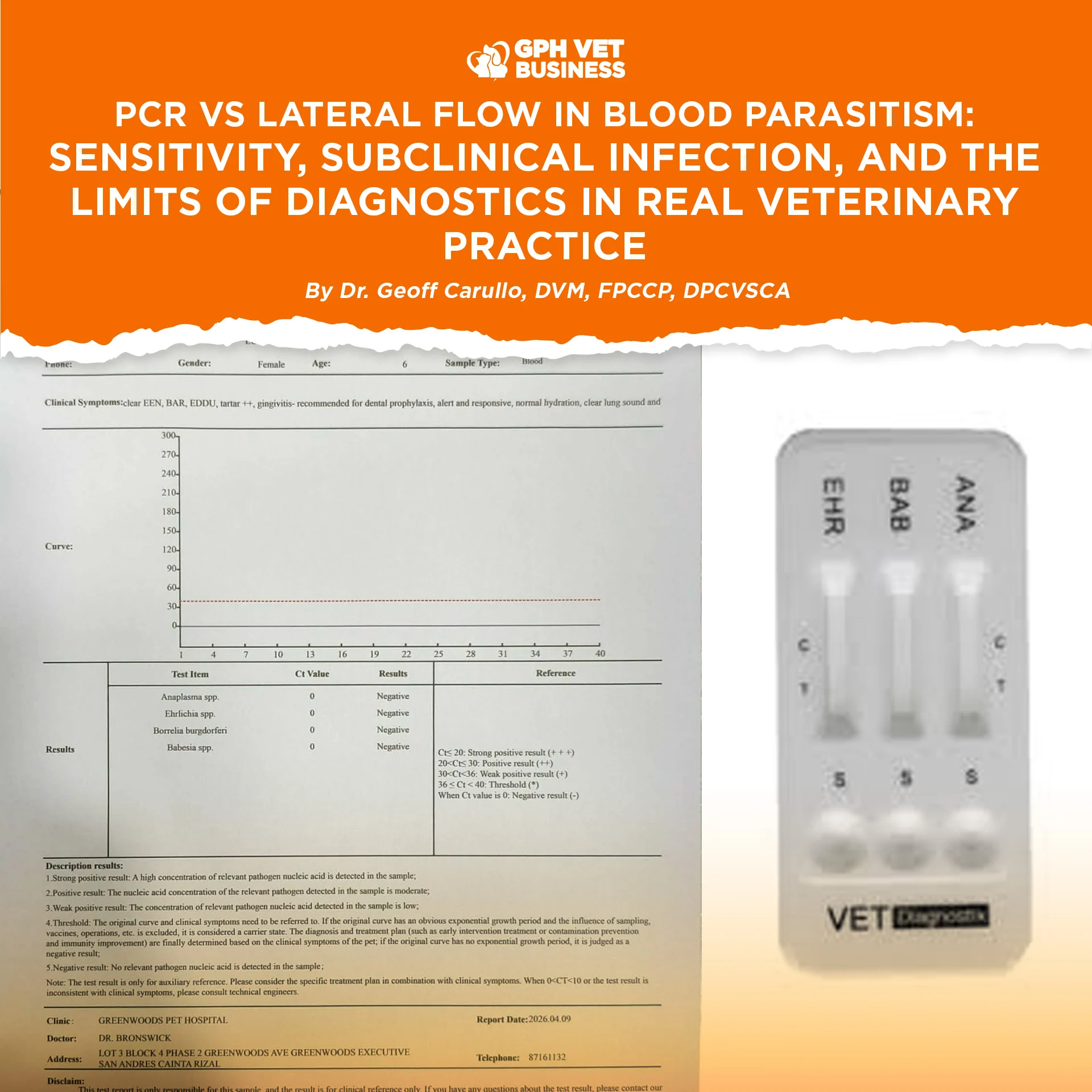
– PCR detects parasite DNA, representing organism presence at the time of sampling
DIAGNOSTIC MODALITIES
Polymerase Chain Reaction (PCR)
Detects parasite nucleic acid (DNA) in blood.
Strengths:
- High analytical sensitivity
- Detects low parasitemia
- Useful in early infection
- Species-level identification
Limitations:
- Requires circulating organisms
- False negatives in low or intermittent parasitemia
- Affected by sample quality and inhibitors
- Higher cost and limited accessibility
Lateral Flow Assays (Rapid Test Kits)
Primarily detect:
- Antibodies (Ehrlichia, Anaplasma, Babesia)
- Occasionally antigens (Dirofilaria immitis)
Strengths:
- Rapid results
- Affordable
- No specialized equipment
- Suitable for routine clinical use
Limitations:
- Lower sensitivity vs PCR
- Antibody persistence after infection
- Potential cross-reactivity
DISCORDANT RESULTS: UNDERSTANDING THE PATTERN
Lateral Flow Positive, PCR Negative
Common in ehrlichiosis.
Possible explanations:
- Persistent antibodies after prior exposure
- Subclinical or chronic infection
- Organism sequestration
- PCR sampling limitation
Lateral Flow Negative, PCR Positive
Seen in:
- Early infection (pre-seroconversion)
- Low parasite burden
PCR detects infection before immune response is measurable.
SUBCLINICAL AND SEQUESTERED INFECTION
In diseases such as Ehrlichia canis:
Acute phase → circulating organisms
Subclinical phase → reduced parasitemia
Chronic phase → localization in bone marrow and spleen
This reflects the concept of:
– pathogen sequestration
Diagnostic Implications
- PCR may be negative if organisms are not in peripheral blood
- Antibody tests may remain positive despite low or controlled infection
Thus:
– Negative PCR does not exclude infection
– Positive antibody test does not confirm active disease
CLINICAL INTERPRETATION FRAMEWORK
Accurate diagnosis requires integration of:
1. Hematologic Findings
- Thrombocytopenia
- Anemia
- Pancytopenia in chronic cases
2. Clinical Context
- Tick exposure history
- Endemic environment
- Recurrence of signs
3. Diagnostic Trends
- Serial CBC monitoring
- Repeat testing when necessary
4. Therapeutic Response
In selected cases, response to treatment supports presumptive diagnosis.
PRACTICAL APPLICATION IN REAL-WORLD SETTINGS
In many veterinary practices:
- PCR is not readily accessible
- Cost limits routine use
Under these conditions:
– Lateral flow assays serve as frontline screening tools
– Clinical judgment becomes central to decision-making
DISCUSSION
PCR is often described as “superior” due to its analytical sensitivity.
However:
– Sensitivity alone does not define clinical utility
Diagnostic accuracy depends on:
- Stage of infection
- Parasite distribution
- Host immune response
- Sampling limitations
No single test provides complete certainty across all disease phases.
CONCLUSION
PCR and lateral flow assays are complementary tools.
PCR excels in detecting low-level and early infections
Lateral flow tests provide rapid, accessible clinical guidance
In subclinical and chronic infections, both have limitations.
FINAL POINT
Blood parasitism is not diagnosed by a single test.
– It is diagnosed through clinical reasoning supported by diagnostics
Not dictated by them.
REFERENCES
- Harrus S, Waner T. Canine monocytic ehrlichiosis: pathogenesis and diagnosis
- Neer TM. Ehrlichiosis: chronic phase and bone marrow involvement
- Irwin PJ. Canine babesiosis: epidemiology and diagnosis
- Otranto D et al. Vector-borne disease diagnostics in dogs
- ESCCAP Guidelines: Control of vector-borne diseases
- PLOS ONE: Limitations of PCR in low parasitemia infections
Dr. Geoff Carullo is a Fellow and the current President of the Philippine College of Canine Practitioners.
Sharing this helps others understand what it really means to be a vet. If you found this valuable, like and follow for more insights.