Why This One Number Still Carries So Much Weight
Every veterinarian has faced this moment. A coughing dog. A hazy thorax. A client asking the dangerous question, “Doc, enlarged ba ang heart?”
Before echo. Before referrals. Before treatment plans.
One number often sets the tone of the entire conversation.
That number is the Vertebral Heart Score.
VHS looks simple. Almost too simple. But when measured and interpreted correctly, it quietly guides decisions that affect diagnostics, cost, urgency, and even prognosis. When used carelessly, it does the opposite.
This article is not about memorizing numbers. It is about using VHS with intention, discipline, and clinical maturity.
What VHS Really Is
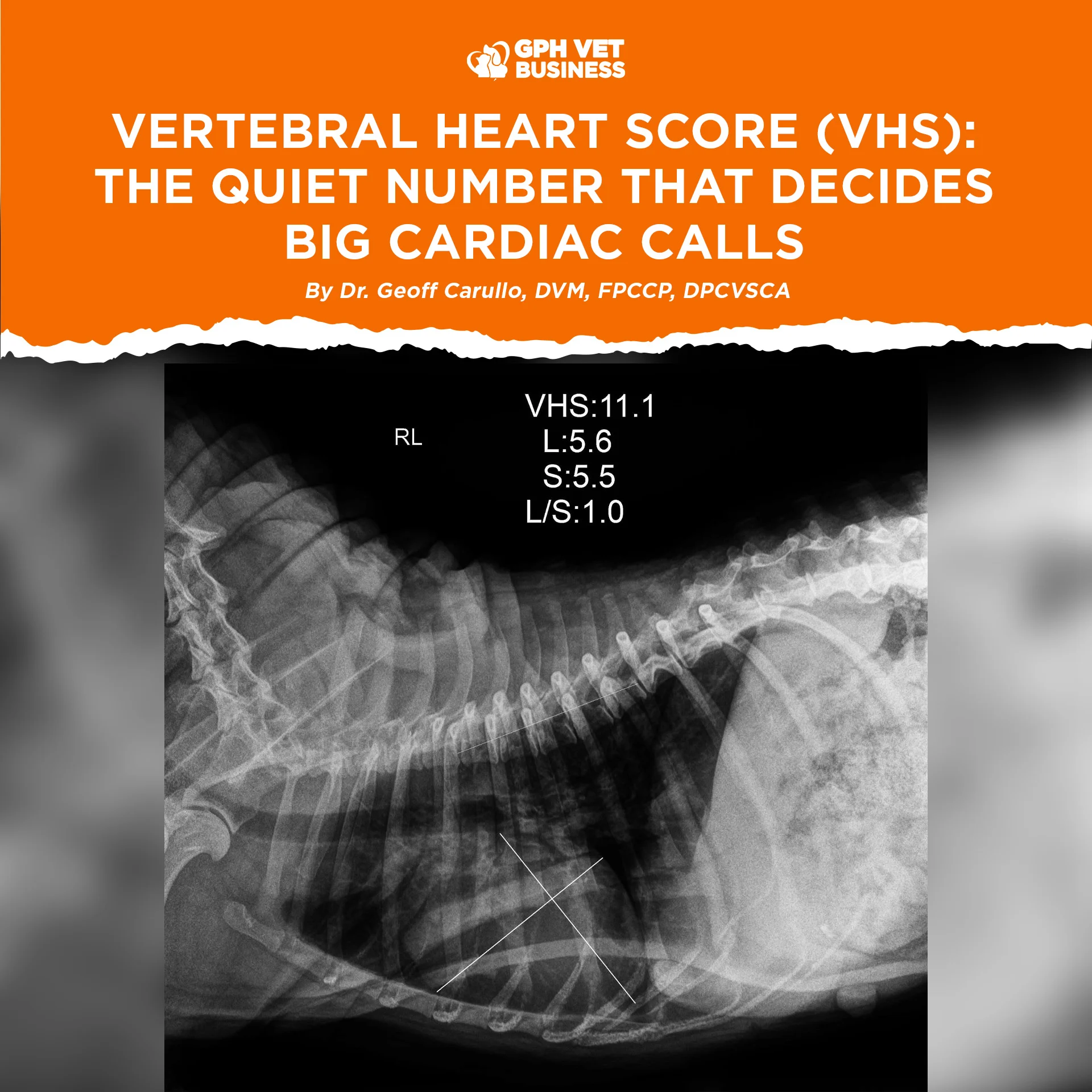
VHS is an objective radiographic method that expresses cardiac size in relation to vertebral length. Instead of guessing whether a heart “looks big,” we translate its dimensions into vertebral units starting at T4.
It does not diagnose heart disease.
It answers a single, powerful question:
Is the heart enlarged relative to this dog’s body size?
That question alone can change everything.
How to Measure VHS Without Lying to Yourself
Radiographic View
- Right lateral thoracic radiograph
- Full inspiration whenever possible
- No rotation. No shortcuts.
Step 1: Long Axis (L)
From the carina to the apex of the heart
Step 2: Short Axis (S)
Widest portion of the heart, perpendicular to the long axis
Step 3: Vertebral Conversion
- Transfer both measurements onto the vertebral column
- Start at the cranial edge of T4
- Count vertebrae spanned
VHS = L + S
Simple steps. Zero excuses for sloppy technique.
The Numbers Everyone Quotes and Few Truly Understand
General Reference Range
- Mean normal VHS: 9.7 ± 0.5 vertebrae
- Values above 10.5 suggest cardiomegaly
But here is the truth many forget.
There is no universal normal.
Breed matters. Conformation matters. Chest depth matters.
- Brachycephalics often run higher
- Deep-chested breeds often run lower
- Cavaliers can look “normal” even with early disease
If you apply one cutoff to all dogs, you are not being objective.
You are being lazy.
Reading VHS Like a Clinician, Not a Calculator
A VHS value should never stand alone.
Always interpret it with:
- Clinical signs like cough, dyspnea, exercise intolerance
- Pulmonary vessels and lung patterns
- Shape of the cardiac silhouette
- Previous radiographs if available
A VHS of 10.8 in a coughing dog with pulmonary edema is loud.
A VHS of 10.8 in an asymptomatic brachycephalic dog may be quiet.
Context decides the volume.
Where VHS Shines the Brightest
Screening Tool
First hint that cardiac disease may be present
Monitoring Tool
Serial VHS tells a story no single radiograph can
Progression matters more than isolated values
Decision Tool
- Helps justify echocardiography
- Supports treatment escalation
- Grounds difficult client conversations in objective data
Common VHS Mistakes That Cost You Credibility
Poor Positioning
Rotation inflates heart size. Incomplete inspiration lies.
Wrong Vertebral Start Point
Starting caudal to T4 falsely increases VHS.
Breed Blindness
Numbers without breed context lead to overdiagnosis.
Overconfidence
VHS does not replace echocardiography. It opens the door to it.
VHS vs Echocardiography: Know Their Roles
VHS asks one question.
Echocardiography answers many.
Use VHS to decide when to investigate further, not to pretend you already know the diagnosis.
Good clinicians know the limits of their tools.
Great clinicians respect them.
Final Thoughts From the Reading Room
VHS is not outdated.
It is not simplistic.
It is not optional.
It is a discipline.
Used properly, it sharpens judgment, protects credibility, and improves patient care. Used casually, it becomes noise disguised as science.
The difference is not the ruler.
It is the veterinarian holding it.
Sharing this helps others understand what it really means to be a vet. Like and follow if you’re with us.